
Mental Illness - Anxiety disorders
Anxiety, the unpleasant feeling of fear and apprehension, is something that most people experience at one point or another in their lives. People have anxious feelings about taking tests, speaking in public, interacting with the opposite sex, making new friends and acquaintances, traveling to strange places, or personal situations (for example, money, job, family, etc.). Anxiety of this nature is completely normal, as long it does not prevent people from going ahead and doing these activities anyway, facing their minor fears or worries and moving forward.
Sometimes, though, some people find that they are paralyzed by their anxiety about a situation or a thing and cannot act. Instead of doing what they know they should, they retreat and avoid the situation entirely. This might not seem too harmful if it is a case of a person being afraid, for example, of tigers. As long as he or she doesn't live in an area populated by such animals, the situation might never present a problem. However, what happens if individuals have extreme anxiety in social situations to the point that they avoid interacting with others entirely? Or, what if people are so afraid of germs that they cannot stop compulsively cleaning themselves to the point that they are unable to engage in normal activities for fear of contamination? It is at this point that individuals must seek professional help in order to conquer their fears so that they can live normal, full lives.
Phobias
Phobia is a form of an anxiety disorder that involves intense and illogical fear of an object or situation. Usually, the individual is aware that the fear is out of proportion to the danger of the thing they fear. In other words, someone being afraid of skydiving or rock climbing wouldn't have a phobia; both of these activities carry high risks for injury or death. However, someone who has never had a negative experience with a dog but is afraid of dogs has a phobia. And, even allowing for the fact that a person has had a negative experience with the thing or situation feared, the presence of a phobia is indicated if the level of fear is out of proportion with the threat the situation or object presents.
The most common phobia is agoraphobia, the fear of public places. This is a phobia that can impair a person's ability to connect with others, to attend
school, and to hold a job. People with severe agoraphobia will not only avoid crowds and busy places, some may refuse to leave their homes entirely. Other common phobias include the fear of heights, called acrophobia, and claustrophobia, which is the fear of closed spaces (such as elevators or overly crowded rooms that leave little personal space).
TREATMENTS. Treatments for phobias usually involve confronting the fear in some way. Behavioral therapists (see Chapter 15: Mental Health Therapies) may use a variety of techniques that involve visualization or actual contact with the object or situation around which the phobia centers. The thinking behind this, for certain schools of therapies, is that it will desensitize the phobic to the phobia. For example, flooding, a behavioral technique, involves exposing a phobic person to the cause of the phobia in an extreme way; however, this can cause the phobic serious initial discomfort, at the very least, and many therapists shy away from therapies that could potentially traumatize a patient.
Operant conditioning is also used in similar ways. Cognitive therapists will work with phobics using cognitive therapies alone (without some type of exposure to the source of the phobia), but this is usually effective only in the case of social phobics. Furthermore, social phobics have responded well to behavioral techniques that involve acquiring better social skills so that they feel more comfortable in social situations. Drugs have also been used to lessen a phobic's anxiety but drugs only mask the fear and will not solve the problem in the long term.
WHAT ARE YOU AFRAID OF?
For every fear, it seems there is a phobia. Listed below are just some phobias, from the common to the plain weird.
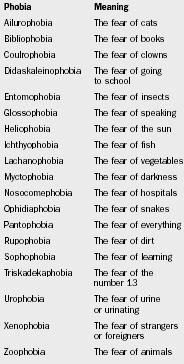
| Phobia | Meaning |
| Ailurophobia | The fear of cats |
| Bibliophobia | The fear of books |
| Coulrophobia | The fear of clowns |
| Didaskaleinophobia | The fear of going to school |
| Entomophobia | The fear of insects |
| Glossophobia | The fear of speaking |
| Heliophobia | The fear of the sun |
| Ichthyophobia | The fear of fish |
| Lachanophobia | The fear of vegetables |
| Myctophobia | The fear of darkness |
| Nosocomephobia | The fear of hospitals |
| Ophidiaphobia | The fear of snakes |
| Pantophobia | The fear of everything |
| Rupophobia | The fear of dirt |
| Sophophobia | The fear of learning |
| Triskadekaphobia | The fear of the number 13 |
| Urophobia | The fear of urine or urinating |
| Xenophobia | The fear of strangers or foreigners |
| Zoophobia | The fear of animals |
Panic Attacks and Disorder
A panic attack can accompany several different anxiety disorders, so in and of itself, a panic attack is not a separate disorder. Essentially, a panic attack is a short period involving intense feelings of fear or discomfort along with several telltale symptoms. These symptoms include an irregular or accelerated heart rate or a pounding of the heart; sweating, discomfort or pain in the chest; a feeling of choking or not being able to breathe properly; trembling, feelings of detachment, of things being "unreal," and/or of impending doom. People experiencing panic attacks have described feeling as though they would lose control completely or were about to have a heart attack or stroke.
Panic attacks can be caused by certain situations, such as being in a strange place, or while a person is relaxing or even sleeping. If panic attacks continue to occur when there is no apparent stressor (stress-inducing event), an individual might be diagnosed with having panic disorder. Panic disorder is a reasonably common ailment, affecting two percent of men and five percent of women. It may begin in adolescence and the disorder is inherited. Biological theories as to the disorder's origin have been put forth as have theories that suggest that panic disorders and agoraphobia are solely psychological in origin. Furthermore, one set of researchers has even suggested that the agoraphobia that so often coexists with panic disorders isn't really a fear of public places but rather a fear of losing control and having a panic attack in a public place.
Certain drugs, such as antidepressants, have been used to treat people with panic disorder and agoraphobia with some success; however, the drugs are merely a temporary measure as people's symptoms will return when they stop taking the drugs. A better approach in terms of a cure might be methods used by cognitive and behavioral therapists, which have proven to help lessen the severity of the disorder.
Obsessive-Compulsive Disorder
Obsessive-compulsive disorder (OCD) involves obsessions (repeating thoughts, impulses, or mental images that are irrational and which an individual cannot control) and compulsions (habitual behaviors or mental acts an individual is driven to perform in order to reduce stress and anxiety brought on by obsessive thoughts or because individuals believe those behaviors or acts will prevent a certain calamity from occurring [for example, believing that a certain behavior will prevent a car accident]). While almost every person may have behavioral quirks or strong preferences (cracking one's knuckles, or wanting things to be kept neat), obsessions and compulsions are different in that they prevent people from living normal lives because they take up an inordinate amount of time.
Obsessions can include thoughts ranging from a person constantly thinking about becoming "contaminated" with germs and avoiding shaking hands with others because of that fear, to a person being convinced that he has left his front door unlocked. The compulsions accompanying these obsessions can include things such as someone repeatedly washing hands for fear of germs, or checking repeatedly (sometimes a certain number—for instance, three times) to see if they have indeed locked the front door. Unlike preferences, a compulsion is something that is viewed as not being part of someone's personality but rather irrational behavior that a person is unable to stop. Due to the nature of this disorder, it can separate people from others, rendering afflicted individuals unable to participate in everyday activities because their obsessions and compulsions prevent them from doing so.
CAUSES. There are many theories surrounding the development of OCD. Behavioral and cognitive therapists believe that the behaviors and thinking related to OCD are learned and reinforced. For example, a person may have the irrational belief that she has not locked her door; by going back to check whether or not it is indeed locked, she is able to relieve the stress that is related to her worries. Some therapists have also pointed to the fact that a lot of the problem stems from the fact that those suffering from OCD simply cannot remember whether or not they did something. There can also be organic (relating to the body) causes for OCD, such as head injuries and brain tumors as well as chemical imbalances in the brain.
TREATMENTS. Treating OCD is not an easy task. One of the most successful therapies involves placing a person in a situation that usually triggers his anxiety, but the patient is not allowed to engage in the compulsive behavior that is the typical response. The idea is that eventually the stress from not performing the compulsive behavior will lessen over time to the point where the person no longer feels compelled to do it.
Prescription drugs have also proven successful in reducing a person's obsessive thoughts and compulsive behaviors; this approach will not necessarily resolve the problem entirely but will free a person to live a normal life while confronting the issues appropriately through therapy.
Post-Traumatic Stress Disorder
Every day, people experience traumatic events, anything from being in a car accident to being robbed or even witnessing such an event happening to someone else. While people may survive these events (which involve intense fear and a feeling of helplessness), and their physical wounds may heal, they can still carry emotional scars. When an individual experiences emotional aftereffects from a traumatic event days, months, or even years after the actual event, this is known as post-traumatic stress disorder (the prefix "post" means after or later). Many of these individuals, even much later, will relive the event, become extremely upset and/or have nightmares about the event. They will also try to avoid things that remind them of the trauma. Finally, they may also be plagued by sleep disruptions, have difficulty concentrating, and startle easily and dramatically.
Post-traumatic stress disorder received a great deal of attention in the years following the Vietnam War (1954–75), as it had after World Wars I (1914–17) and II (1939–45), the Korean Conflict (1950–53) and, in fact, even after earlier conflicts such as the American Civil War (1861–65), because of the emotional scars that those who had served in a war often seemed

to display. In fact, PTSD was originally called "shell shock" (in reference to the ammunition used during times of war). It is now known that those who have witnessed or participated in any type of traumatic event—such as being involved in the search-and-rescue or recovery missions for the victims of plane crashes in which hundreds of people perish—are now known to be potential sufferers from PTSD. What is mysterious about PTSD is why it affects only certain people and not all of those experiencing similar events or even the same event.
TREATMENTS. Great strides have been made in treating PTSD through group therapy. Talking in a group to others who have experienced similar events and have been suffering from them continuously can be very helpful because patients can feel that they are not alone in their feelings and that there are people who understand the intensity of their traumatic experience. Most therapies, in groups or single client therapy, usually will involve confronting the event in some way. Stress management and medication have also been used with some success.
People who have lived through traumatic events should be encouraged to seek at least brief therapy to ensure that PTSD won't develop years later.
Comment about this article, ask questions, or add new information about this topic: